Preparation of monitors, oxygen, BVM device with a PEEP valve, suction, endotracheal tubes (ETTs), stylet, laryngoscope and blades, drugs, alternative intubation options and rescue devices should occur. RSI drugs and post intubation sedation medications should be drawn up and immediately available for administration. Note that psychological preparation should be performed with the mentating patient: the patient should be told the rationale for the procedure including the margin of safety maintained and what to expect in a calm, reassuring manner. If possible, the patient's cooperation should be enlisted with mouth opening and tongue protrusion.
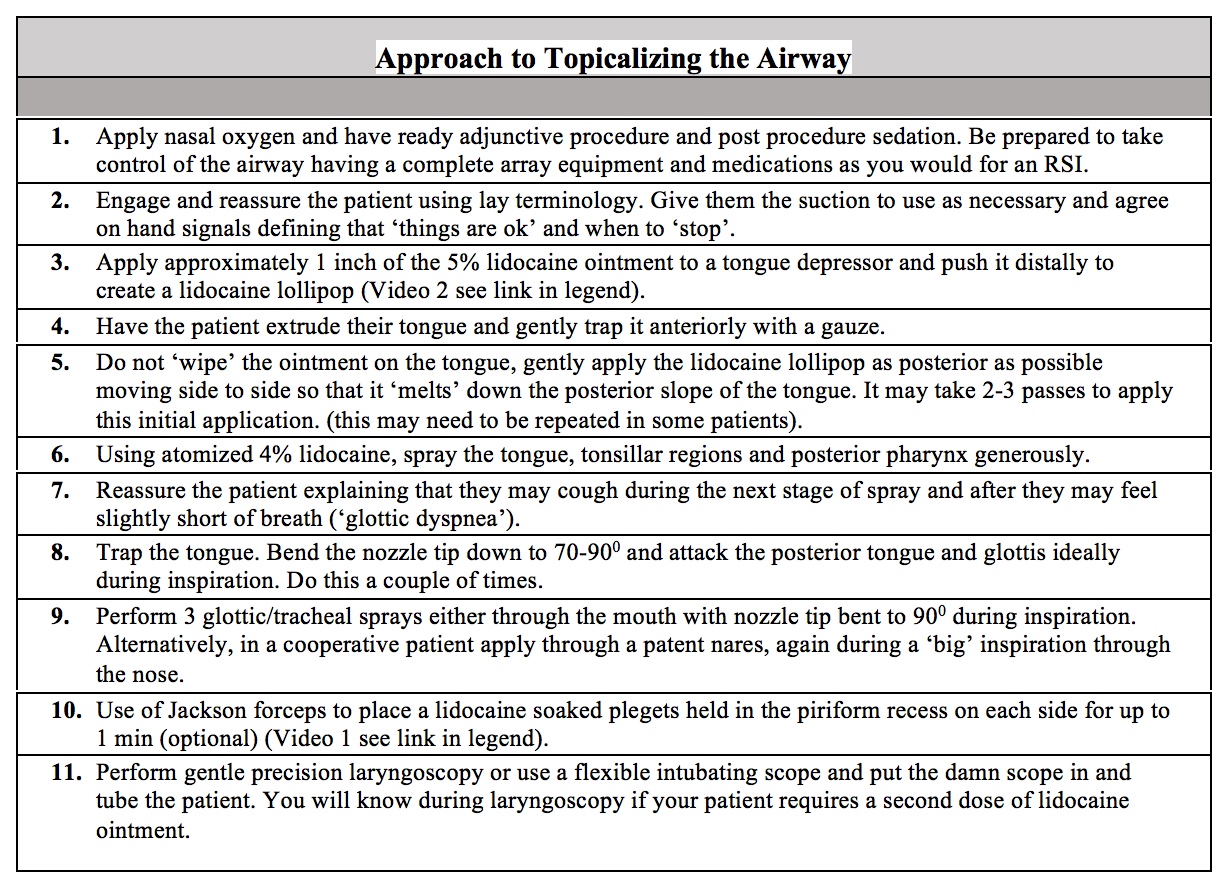
Topical airway anesthesia should be applied, as described above and summarized in table 3. Sedation can be used as necessary, recognizing the goal of maintaining patient cooperation. Topicalization of the upper airway can produce both cough and a sense of dyspnea. This latter effect can cause anxiety in both the patient and operator if it is unexpected. This 'glottic dyspnea' is likely caused by the loss of the normal (unconscious) sensation of respiratory flow across anesthetized vocal cords. It is easily manageable if anticipated.
The tube location is confirmed. Once the patient is intubated, the ETT cuff is inflated. Often, the patient will cough, and expiratory flow can be felt and heard issuing from the proximal end of the tube. The patient should not be able to vocalize. Objective confirmation of placement with waveform ETCO2 capnography is mandatory.[35] The patient should be reassured that the procedure has been successfully completed, and that vocalization will not be possible.
Additional sedation should be provided and adjusted as necessary based on patient hemodynamics. Vital signs should be rechecked.