More on 3 moves to help ETT advancement with hyperacute VL blade use
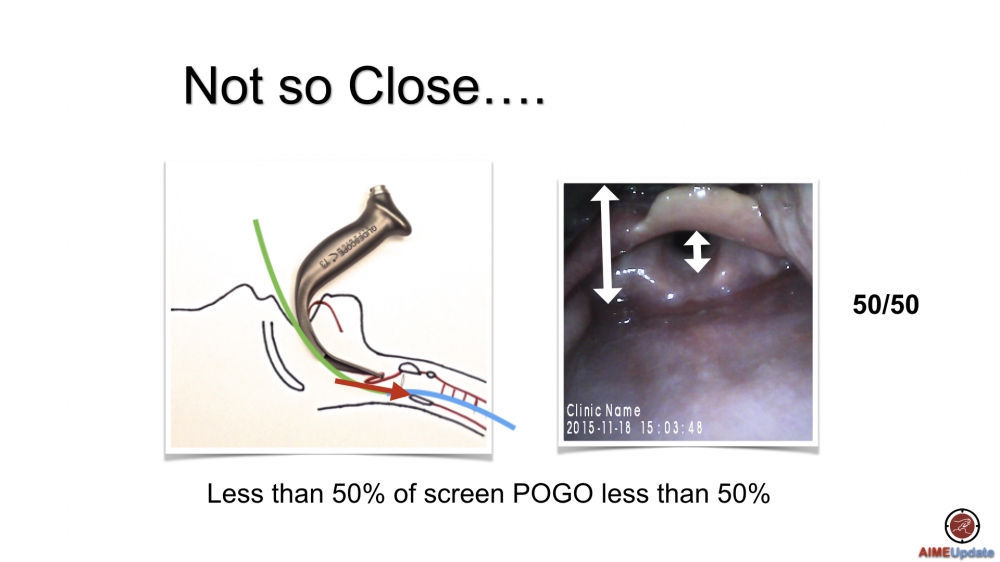
In my last post Too much of a good thing I reviewed the importance of Hyperacute angled (HA) VL blade positioning. Most of the time a deliberately restricted view (50/50) with the blade tip in the vallecula will allow for easy tube passage. However hold up can still occur on the anterior wall of the trachea. In another post on twitter I demonstrated 3 moves to help manage ETI advancement when using a HA-VL blade.
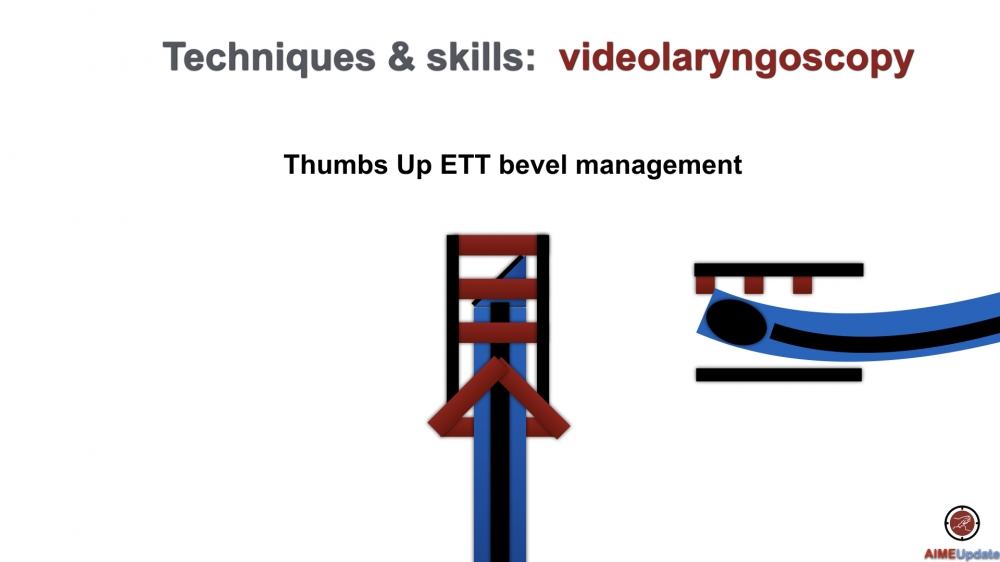
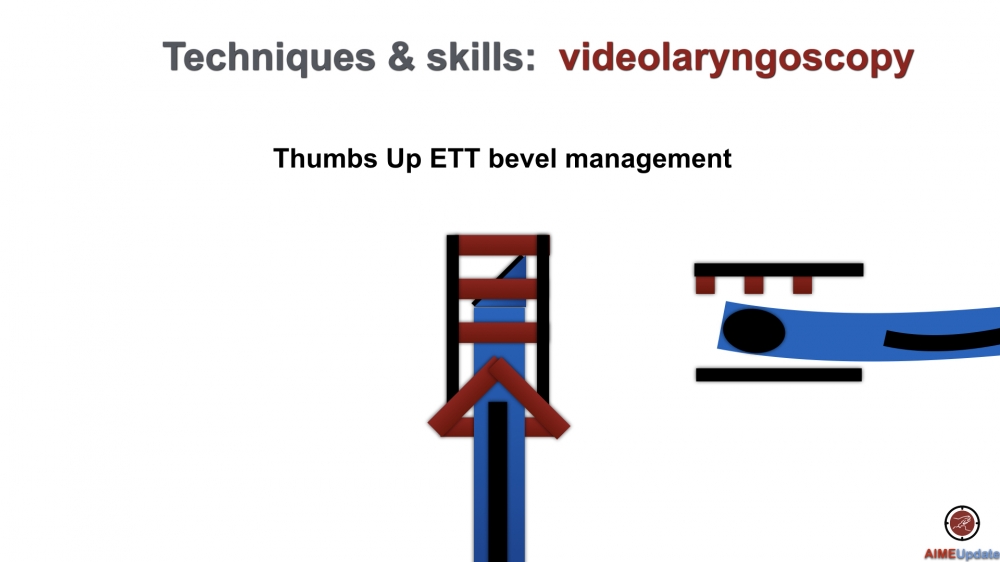
The first move is to partially pull back the stylet by approximately 3 cm. The cuff should be mostly beyond the cords for this to be done safely minimizing the risk of the ETT migrating proximally then inferiorly into the esophagus. I use a stylet straight-to-cuff and shaped just proximal to the balloon at roughly 60-70 degrees (see how to shape your stylet). Any more of a bend makes anterior tracheal wall hang-up more likely. To easily perform a controlled partial withdrawal of the styleted ETT yourself, the proximally protruding end sitting above the connector should be bent 90 degrees allowing a thumbs up maneuver. This has 2 effects: one it causes the distal end of the ETT to straighten and secondly it allows portion of the tube to flex against the anterior tracheal wall facilitating advancement.
Fig: leading edge of ETT with fully engaged stylet caught anterior on tracheal ring. Normal position of open face of bevel is to the left.
Fig: Partially rertracting the stylet potentially softens and straightens the dital ETT
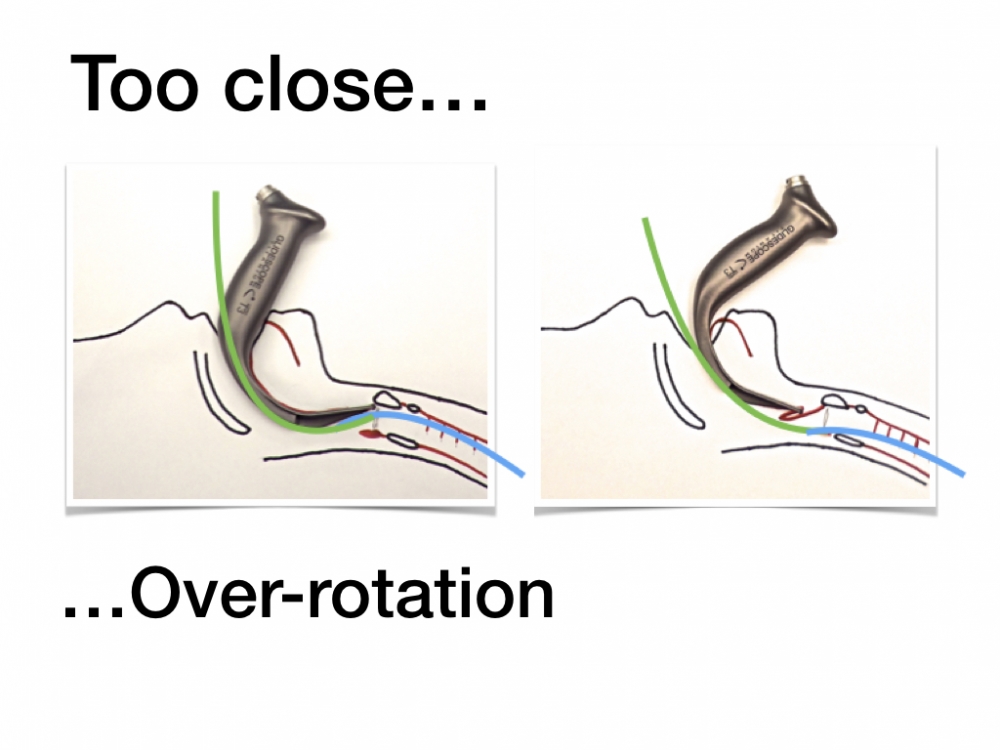
The next move I would try is to relax the distal end of the VL blade. The curved shape of HA-VL can cause a rotational force that deflects the proximal trachea anteriorly creating a more acutely opposing angle between the glottic inlet and the long axis of the trachea. This effect is more pronounced when the blade tip is closer to the glottis. In fact it is my contention that the 50/50 restricted view exerts its beneficial effect by causing the blade to de-rotate.
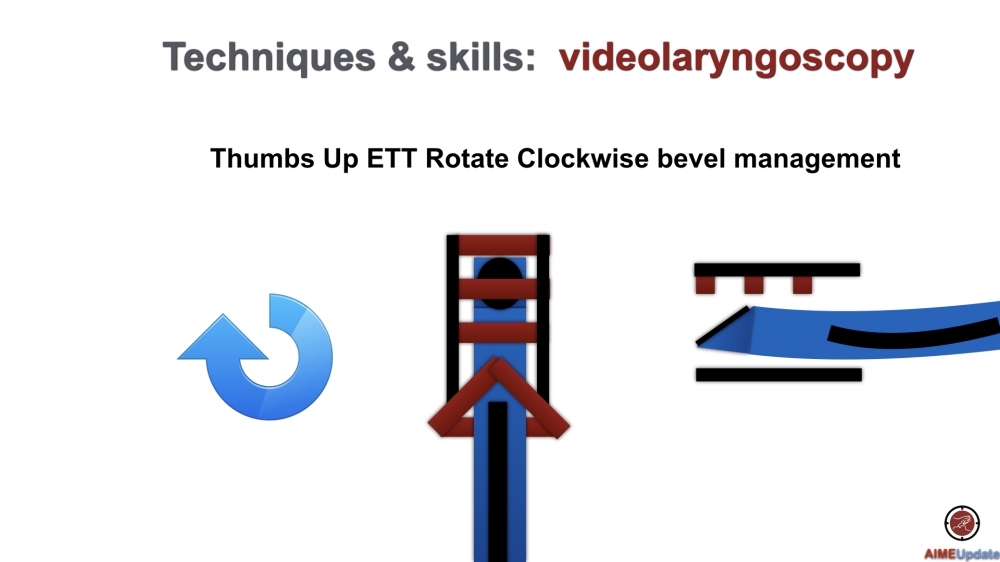
Lastly if the ETT still won’t advance then rotate the ETT to the right (clockwise) ie drop it to the bed. This takes the leading edge of the bevel off the tracheal wall positioning the more favourably oriented open face of the bevel anterior. In addition it puts the distal bent (shaped) portion of the ETT in the same long axis as the trachea.
Fig: Rotation clockwise 90 degrees takes the leading edge off the anterior wall positioning the open face of the bevel anterior.
Check out more of an explanation here: Twist and shout. If there is continued hold up, continued rotation clockwise to 180 or more takes the distal curve of the ETT posterior (the trachea runs from a proximal anterior position to a distal posterior position), freeing up the the ETT for advancement.
If the above hasn’t worked, good old fashion DL or Mac VL may be your answer once you’ve reoxygenated the patient.